
SHARE UBT Fair Wednesday! Plus, Your AFSCME Benefits
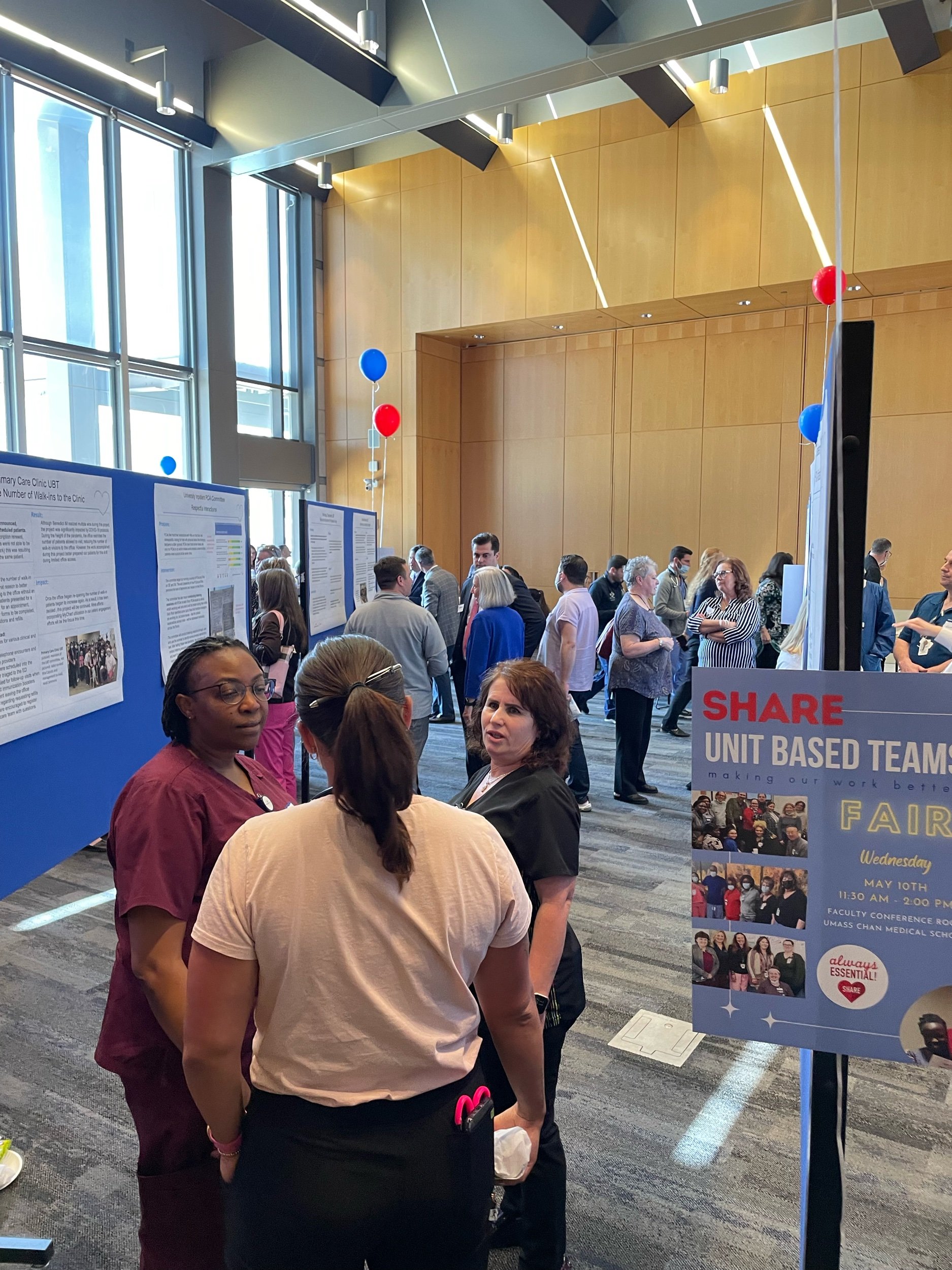
Wednesday is the big day. SHARE members are making it easier to give great patient care. If you’re on the University Campus, come celebrate your successes and those of your co-workers. Plus, enjoy a Regatta sub sandwich. Hope to see you there!
About Your AFSCME ID Card
It’s time again: new AFSCME Union ID cards have begun arriving in the home mailboxes of SHARE members. Why did I get this? you might wonder. What is it good for?
Keep track of your AFSCME Member Number to take advantage!
AFSCME is SHARE’s parent union. (SHARE is also known as AFSCME Local 3900.) And, your Union membership comes with perks. Nationwide, AFSCME represents over a million members. That creates a lot of leverage in negotiating deals on things such as:
And there’s much more. Visit the Union Plus website to explore the good things available there.
For some of those deals and services, you may need to provide your union local number, and your personal union member number, which are both printed on the card. If you don’t receive a membership card in the next couple of weeks and need your membership number, please contact the SHARE office (508-929-4020). Although we can’t reprint the card itself, we’ll be happy to help you track that down.
Our union takes a very grassroots approach. We’re focused on the issues in our hospital, on working so that SHARE members can always be moving forward financially, and on continually strengthening our community so that we can all do work that we’re proud of. But going out for a cheaper meal can be pretty nice, too.
How To SIGN UP FOR UNION PLUS
It’s easy. Visit www.unionplus.org.
On most browsers, you can find the “sign up” link in the upper right-hand corner.
When selecting your union from the dropdown menu, please choose “AFSCME (State, County, and Municipal Employees)”
SHARE is also known as AFSCME Local 3900
All SHARE members qualify for UnionPlus benefits
From the Partnership Office: Leveling Up
In case you missed it — and, because we really value the achievements of these teams — we’re reprinting the below article from UMass Memorial’s Hub. Unit Based Teams (or UBTs) are at the core of SHARE’s mission. UBTs are designed to put SHARE members directly in the driver’s seat, designing their own work in the ways that make the most sense. Developing a high-level UBT makes it easier to deliver care to be proud of.
The SHARE UMass Memorial Partnership Office comprises a crack team of Continuous Improvement Coaches, as well as a Program Coordinator. They facilitate UBT meetings, measure the progress, and help find the tools and strategies to get things done. At least, that’s the Coaches’ initial role with each Team. As the Teams develop and mature, they’re more self-reliant . . . and, hopefully, more easily able to find happiness and satisfaction in their work.





UBT Spotlight: Denials and Specialty Billing
The Success Story of the Denials and Specialty Billing UBT
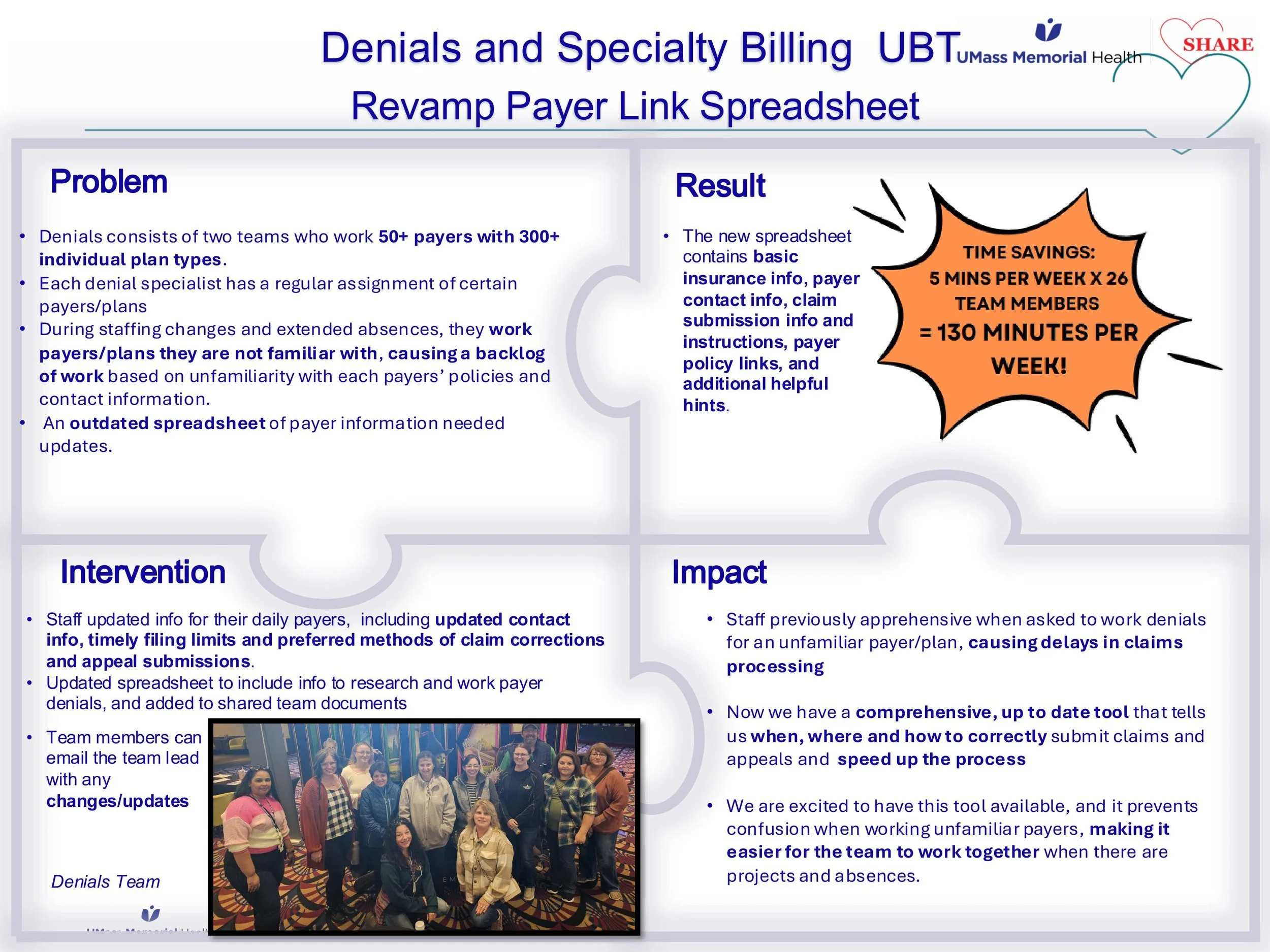
UMass Memorial’s Denials and Specialty Billing Department is “Busy,” as their Director Dan Rossi puts it, “thirteen months out of the year.” And yet, their Unit Based Team (or, UBT) has found a formula for success, one that’s rooted in culture, collaboration, and continuous improvement.

Speaking about their “Finding 4%” project to SHARE members and caregivers from throughout UMass Memorial at a recent UBT Peer Learning Event, SHARE UBT Co-Lead Mary Jacquot joked, “You can all stop looking, we found all of the 4% money right here.”
It was a wry joke, but there’s an important truth underlying it. The Denials team knows that they’re often a last line of defense for recovering money that’s owed to our hospital. Without good systems and good communication, high dollar accounts can time out. A single mishandled claim can amount to hundreds of thousands of dollars in lost revenue or more.
Not every hospital department can reconfigure its processes to eliminate waste in a way that results in as much financial gain, but many of their Team’s successes can be recreated by SHARE members throughout the system, with powerful results.
What Makes This Team Stand Out?
SHARE UBT Co-Lead Mary Jacquot sums up her approach to the work with three words: “open, honest, and unafraid.” Mary’s worked long enough to recognize that fear can stifle progress—fear of managers, fear of looking uninformed, fear of admitting mistakes. She’s seen it in her previous work experience, and works to inspire a different mindset.
The department manager and fellow Co-Lead, Kaitlyn Licht, regularly participates in these meetings, too, along with area Director and Team Co-Sponsor, Dan Rossi. SHARE members on the team credit their current management team’s listening ear and democratic work-style as a major contributor to the team’s positive culture.
Listening to the Front Lines
Even with the most supportive management team, it can sometimes seem harder when “the boss” is looming. But Mary encourages SHARE members to be assertive wherever possible: when at least one brave voice breaks the silence, it paves the way for others.
“Nobody knows everything, and that’s okay. UBT meetings are a safe space where ideas flow freely,” Mary says. When one person speaks up during one of their remote Team meetings, others on the WebEx screen nod in agreement, reinforcing a shared understanding.
Department manager and management Co-Sponsor Kaitlyn Licht emphasizes openness to ideas, especially from those in the trenches. Competing ideas can be tough, she says, but this team embraces the challenge, knowing that innovation often comes from healthy discussion.
Celebrating Wins and Building Trust
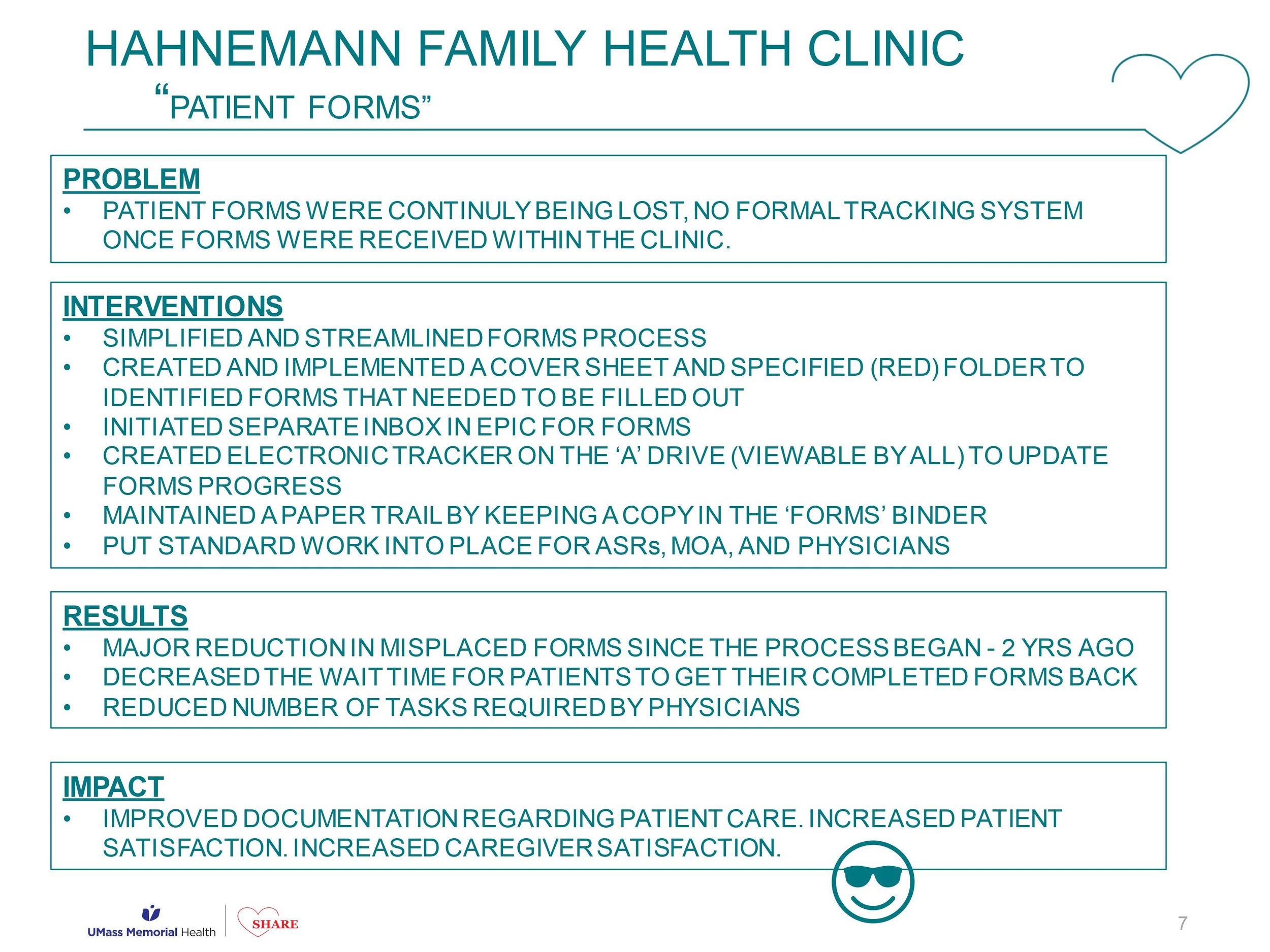
The team recently reached Level 4 on their UBT Path to Performance, which you can see in the below slide-deck, and is aiming to reach the highest step in that path, Level 5—a testament to their commitment to growth. Many members are enrolled in Yellow Belt training, and leaders are stepping up by taking programs such as Leading at the Speed of Trust.
Gratitude is also woven into their culture: department notes with kudos and recognition through UMatter keep morale high. While UMatter entries go into staff files, the real magic is in how this team regularly celebrates one another.
At a recent Labor-Management Partnership Council meeting, Dan Rossi admitted that they’re not formally tracking all their improvements the way that they used to, but that’s only because the continuous improvement cycle has become so engrained in their workflows that it’s second nature.
The team’s progress is tracked and cheered on by Jackie Zhou, a Continuous Improvement Coach in the SHARE/UMass Memorial Labor Management Partnership Office. “We are incredibly proud of the team for reaching their Level 4 UBT milestone,” she says. “After coaching this UBT for the past two years, I’ve witnessed a powerful culture shift in the last year. Continuous improvement has truly become second nature, and every team member is empowered to bring forward ideas and turn them into real solutions. Keep it up!”
Looking Ahead
Opportunities like the Seed Grant are on the horizon. Kaitlyn’s idea to use it for multilingual patient letters—especially Portuguese—shows how this team thinks beyond the immediate task to improve patient experience.
The Secret Sauce?
The example set by Denials and Specialty Billing isn’t just a method for reaching status as a Level 4 UBT — it’s a formula for success.
Of course, formulas only go so far. But! We know if we could bottle it up their secret sauce, it would contain a few key ingredients:
Fearless communication: Open, honest, and unafraid.
Shared accountability: Everyone on the same page.
Ongoing improvement: Measuring what matters.
Continuous learning: Certifications and leadership programs.
Culture of gratitude: Celebrating each other’s contributions.
Congratulations to this UBT for reaching Level 4! We’re grateful to the whole Denials and Specialty Billing Department for the work you do to keep the revenue flowing to our hospital, and for setting a beautiful example of what good communication and teamwork can do.









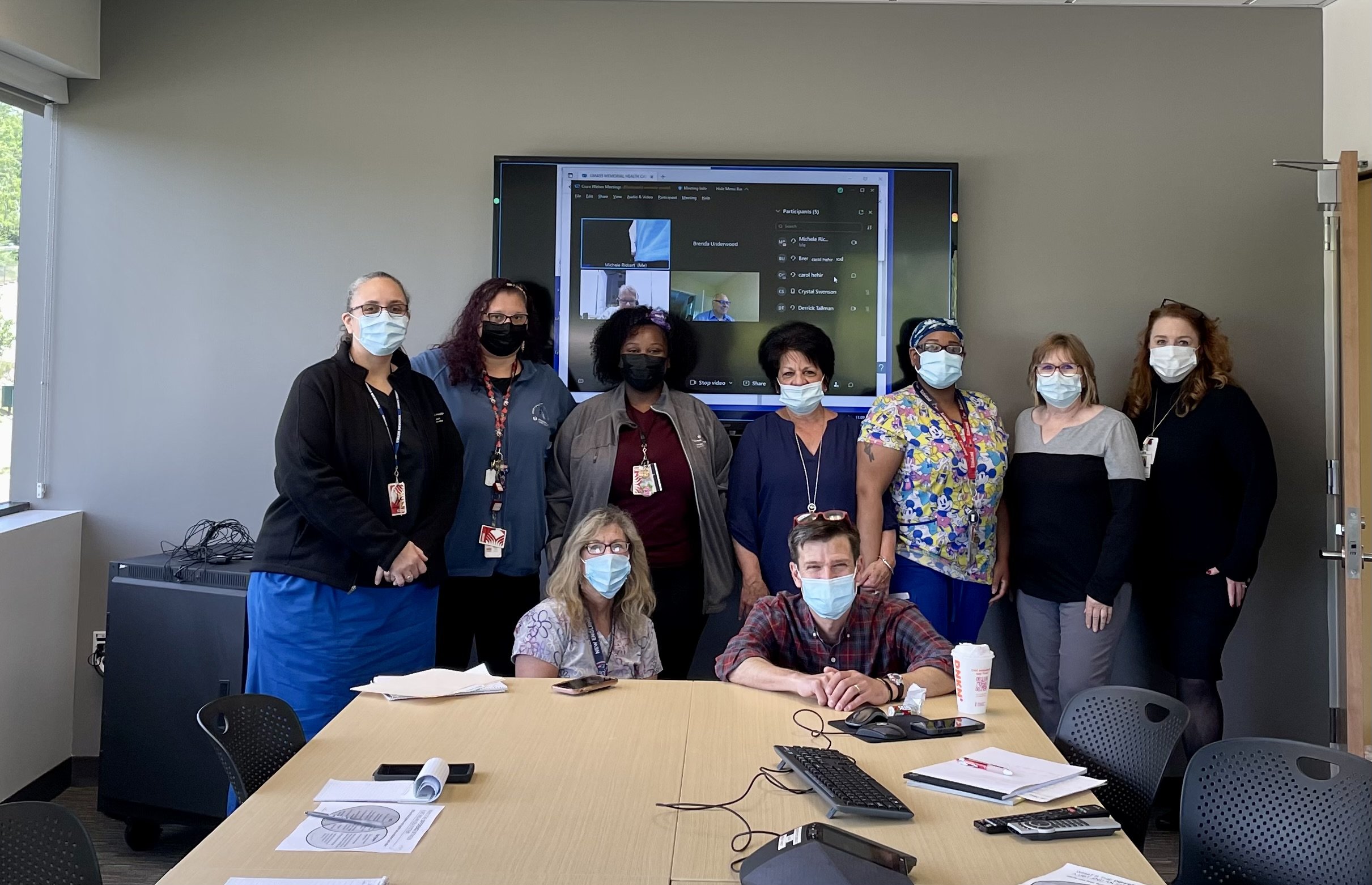
Memorial UBT Fair TODAY
If you’re at the Memorial campus today, we encourage you to head down to Knowles Hall in the Jaquith building during your lunch break to check out the two dozen posters presented by SHARE UBT Co-Leads . . . and enjoy a complimentary sub sandwich. There will be a short, festive presentation just after noon. See you there!

Hahnemann Campus UBT Fair: Wednesday, May 7, noon-1pm
Our celebration of Unit Based Teams continues . . . with the first-ever UBT Fair at Hahnemann!

University UBT Fair: this Wednesday, April 23
Please join us for lunch at the 3rd Annual UBT Fairs!
Beginning this Wednesday, the Labor Management Partnership Office, together with the SHARE union, will be hosting the 3rd Annual UBT (Unit-Based Team) Fairs!
These drop-in events are open to all caregivers.
Come grab lunch provided by SHARE, enter a raffle, and see how your fellow caregivers have improved their own work through the UBT projects they designed and implemented.
2025 UBT Fair Locations
University campus: Wednesday, April 23rd 11:30-1:30 in the Faculty Conference Room in the Medical School
Hahnemann campus: Wednesday, May 7th 12:00-1:00 in the Hallway leading to the Cafeteria
Memorial campus: Thursday, May 22nd 11:30-1:30 in Knowles Hall in the Jaquith Building
Featuring: Lunch, raffles, SHARE and other organizational leaders, friends, and fun!
Sponsored by the Labor Management Partnership Office & the SHARE union.
Please feel free to reach out to alaina.anderson@umassmemorial.org with any questions!
click the above or below poster for a printer-friendly version to post in your department









2024 IHI Conference Presentation: Unit Based Teams
Ever wonder exactly what’s getting said outside our hospital about the work you do? Continuous Improvement Coach Will Erickson had the following to say to healthcare leaders from around the country in a talk that he gave at the recent Institute of Healthcare Improvement Conference in Orlando, Florida . . .
IHI 12/10/24

Will Erickson presenting at IHI in his trademark red sweater. To see the slides from his presentation, [[[click here]]]
I’m Will Erickson, I work as an organizer and continuous improvement coach with the Labor Management Partnership Office at UMass Memorial Health in Worcester, MA. I’ve attended the Forum several times over the years but this is my first time presenting, and I’m so grateful that my friends Amar and Becka invited me to join them.
Ok, so now I’m going to tell you about how we’re improving how people feel about coming to work every day through our Unit Based Team program at UMass Memorial, in partnership with our largest union.
First, a little bit about our system: we’re a mid-size academic medical center and safety net with a bunch of community hospitals and practices in Central Mass. We’re the largest provider and largest employer in our region, so the quality of our jobs, and our care, really matters to our community. Unless I’m misjudging this audience, I’ll bet a lot of you work in places like this one.
To understand this story you also need to know about the SHARE union, which makes up the other half of our labor management partnership. It’s the largest union because it represents a lot of different job titles, like nursing assistants, medical assistants, rad techs, respiratory therapists and billers. We organized our union around the values of solidarity and voice: taking good care of each other and being able to participate in decisions about what happened to us. I say us because I come out of this union as an organizer. The lead organizer of that union, Janet Wilder, is in the audience this morning.
Coming into 2016, SHARE leaders had achieved a lot in terms of making their jobs better, but they felt that they hadn’t made a lot of progress making these jobs feel better – in a lot of ways, the work felt harder and more draining than it had. Together with UMass Memorial, we found ourselves facing a shared set of problems; a disengaged workforce that resisted changes they perceived as being done to them – no one wants to feel process improved. We suffered from unreliable processes and variable outcomes, pretty bad patient experience scores, and strained labor relations. And that’s a picture of a much younger me manning an informational picket line in front of one of our hospitals, just to prove my labor bonafides.
We looked around for alternatives, and found the Kaiser Permanente Labor Management Partnership, which is still in place today and the most important labor management partnership in place in US healthcare right now, maybe in any industry in the US. With support from Kaiser and its unions, from our own hospital’s leadership which was a couple years into a Lean journey, and drawing inspiration from a couple trips to the IHI Forum, we did something brave and formed our own labor management partnership, one that was built on those central pillars of voice and solidarity, participation and mutual respect and support.
Following the lead of our friends at Kaiser, our Unit Based Teams are built on the foundation of this labor management partnership. These are department-level process improvement teams create to help us establish a more invigorating work culture, to make labor management partnership an actual, real thing at the frontline between staff and their managers and not just for the leaders at the top. This is our effort to organize a bottom up social movement for safer, smoother, better processes.
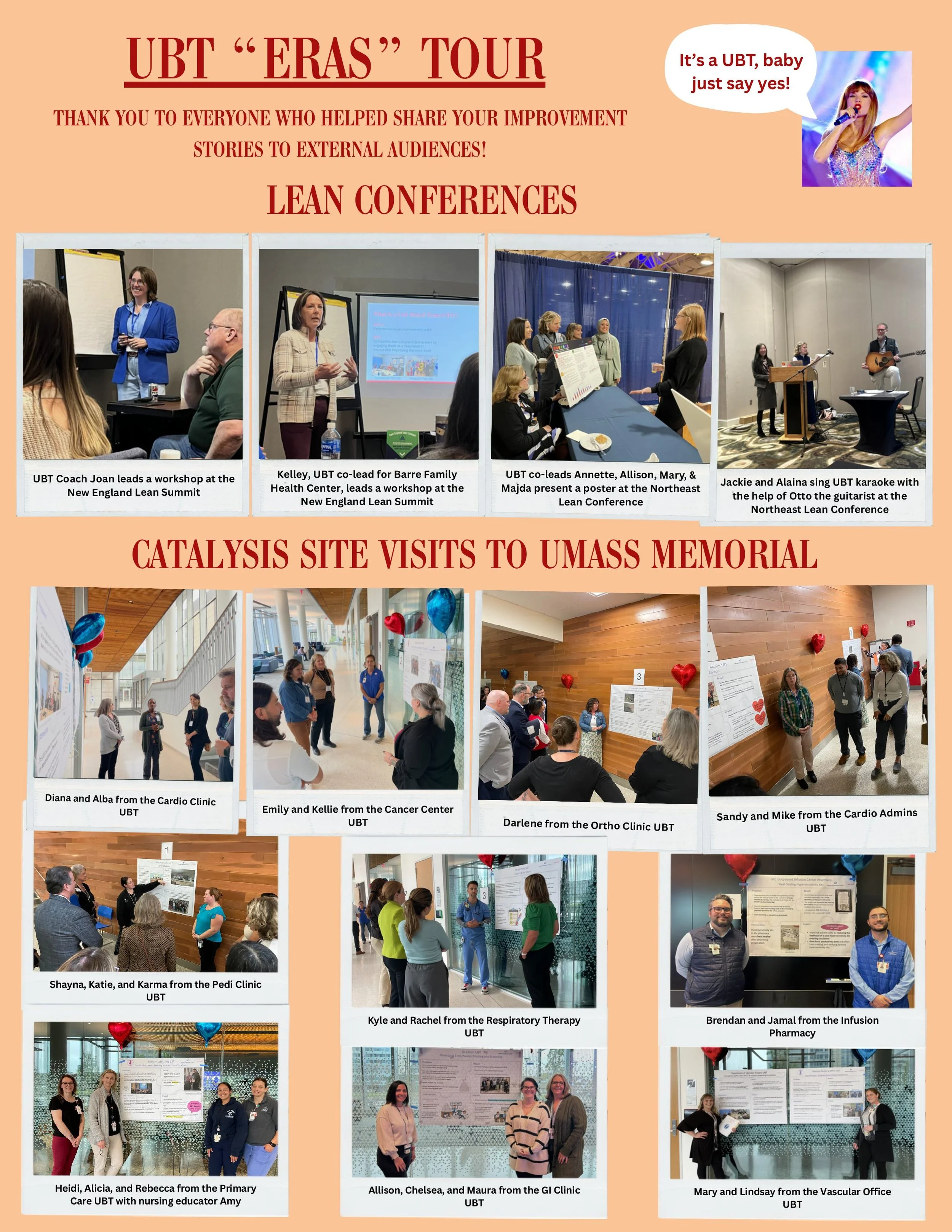
This is a picture of one of our UBT Fairs from last Spring, when we got several hundred of people together to share out posters of their favorite improvement project from the last year. One of the great things about rooting our movement for process improvement in the labor movement is that in the labor movement its still cool to belt out songs together, its one of our proudest traditions. So at these UBT Fairs we actually pass out adapted lyrics to pop songs and get several hundred people to sing together about their love for process improvement.
We now have 70 or so UBTs working on projects to reduce falls, to improve patient experience, to reduce no shows, to improve copay collection, to improve throughput. But the UBTs don’t exist for the purpose of solving those problems. The primary purpose of a UBT is to change how our caregivers feel about coming to work everyday. But the big theory of change that animates this whole program for us is that the best way to change how our people feel about their work isn’t pizza parties, or ropes courses, or trust falls, or meditation apps (we’re not against those things) but to involve our frontline people in identifying and then working to solve the process issues that are driving them the most bananas.
Each UBT has a committee of staff, providers and managers. Each is co-led by a labor co-lead and a management co-lead, and each team, in addition to having an improvement coach like me, is co-sponsored by a union leader and a management leader, usually the manager’s boss.
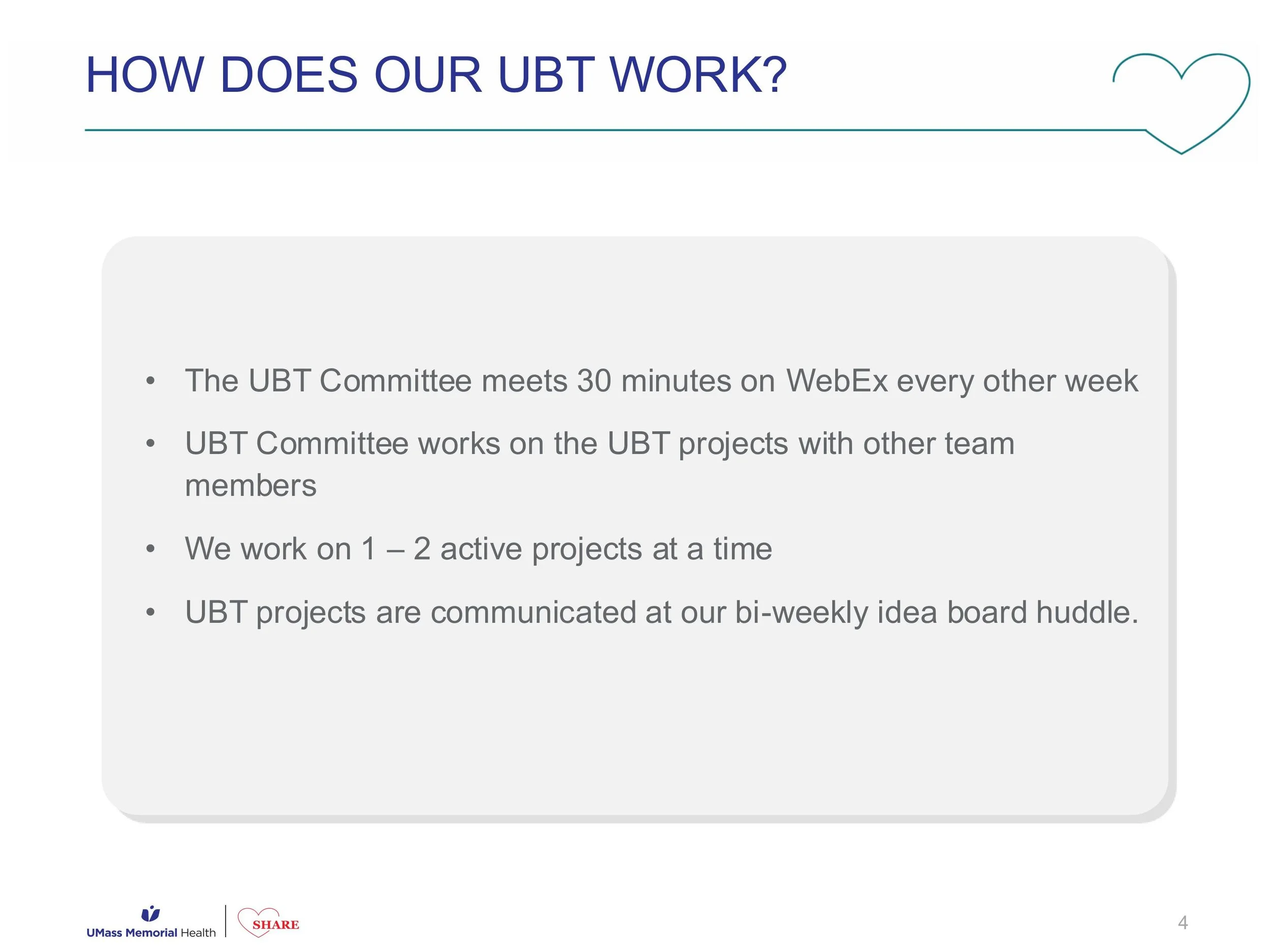
Most of our UBTs meet for 30 minutes every other week, and each works on 2-3 projects at a time. We encourage them to work on big issues, but to scope their project such that it can be completed in less than 100 days – I think that 100 day rule is one we brought back from one of these forums. The co-leads facilitate the meetings and prep for those meetings together beforehand. Our co-leads are really the axle around which the UBT turns, so we give them lots of training and support – we view UBTs as a vehicle for developing frontline leaders and upskilling our managers, not just for process improvement. Projects are chosen by the committee, and decisions are made by consensus. We test for consensus by asking three specific questions: has everyone been heard? Can everyone live with this decision, even if it wasn’t your first or second or third choice – will you try it? And finally, will everyone here support this decision outside this room – are we together in this? We want our improvements to stick.
So that’s the concept, but are they actually making a difference? There are several different ways to answer that question. First, our UBTs are making big, substantive impacts with their projects. One of our CT departments, for example, created a patient staging area and reduced wait times by 20% despite an increase in volume. If the management team had gone to the staff and demanded an increase in volume, the techs would have spit the bit – what stressed the techs out more than anything else was how late they were running pulling in outpatients in the afternoons – the techs wanted to see a decrease in outpatient slots. After setting up the staging area, our techs’ reported stress levels were 40% lower. Happier patients and smoother process made happy techs.
Our managers are also reporting general improvements in productivity and good feeling as a result of their UBT work – a kind of generalized halo effect. I love this quote from one of the NPs in Vascular Surgery – this department started out meeting every other week for 30 minutes, then increased that to every week for 30 minutes, and then they extended the time to a full hour because they felt like they were getting so much out of the time together.
And we’re seeing an effect in our caregiver experience survey results as well. In a recent survey departments with a UBT showed twice the improvement in engagement as our entire system, and four times the improvement in the bundle of questions that basically get at what people think of their boss. And the questions with the biggest gap between departments with UBTs and those without one were “I am involved in decisions that affect my work” and “this organization treats employees with respect”. Remember that we built our partnership on the pillars of increasing participation and improving the culture – I just love that.
Our joint improvement work is also gaining notice in the labor relations universe. Here we are with US Secretary of Labor Julie Su. She’s unfortunately only got a few more weeks in the job.
And of course the best evidence that we’re making an impact is what our caregivers are saying about how UBTs have changed them, and how they feel about coming to work. We’re not going to have time to show you this compilation, but we’ll give you the QR code at the end so that you can watch on your phone – I really hope you will.
So to wrap up, what’s different about these UBTs? First, ownership is truly shared. This is not a top down management thing, but its not just a union initiative either. That’s made it easier to leverage multiple leadership networks, especially our often unsung, informal frontline leaders, and sometimes even those grouches in the department who’ve historically been skeptical of any change. We also think we’ve created a structure that makes it easier to talk about hard things – partnership doesn’t mean that we just act nicey-nice to each other. We don’t tiptoe around the hard stuff. We lean into the process issues that are causing conflict, because we want to solve those things. And finally, with every project, every meeting, we’re teaching our people how to work together better and to solve bigger challenges. We’re doing it in a way that refreshes the manager role, positioning them as mentors and leaders, not just command and control authoritarians. And we’re challenging union reps to not just complain that management hasn’t fixed something yet, but to jump in and organize their coworkers to come up with a better way. And we’re doing it in a way that strengthens psychological safety and combats against of the real power imbalances that can make working in a team so hard.

SHARE UBTs Celebrate Reaching Top Level of Path to Performance
UMass Memorial Health and SHARE leaders recently celebrated an impressive milestone reached by two Unit-Based Teams, or UBTs. A UBT is a frontline-led, department-level improvement system that enables caregivers to work on the process problems that make it hardest for them to feel proud of the care they deliver.

This week, Dr. Eric Dickson and other hospital leaders visited the Vascular Surgery Office and Diabetes/Endocrinology departments to celebrate the teams becoming the first UBTs to reach Level 5 status on the UBT Path to Performance.

While over 75 UBTs have been launched over the last several years across the Medical Center, Medical Group, Revenue Cycle, and Marlborough Hospital, these are the first to have reached this top level of performance.

In order to progress through the Path to Performance, a team, made up of a voluntary group of employees consisting of managers, union organizers, and frontline staff, must demonstrate competence in various ways, with a focus on designing and completing improvement projects in their own department. UBT projects often tackle things such as communication or workflow. The ultimate goal of the UBT is to make their departments better places to work — more enjoyable, smoother running, and easier places to give the high-level patient care that they want to provide.

In addition to delivering to each team a traditional SHARE-UMass Partnership Office award — a balloon shaped like a number “5” — Dr. Dickson heard from caregivers about which UBT projects have meant the most to them, what they are working on now, and how having a UBT has changed how they feel about coming to work.
Congratulations Vascular Surgery Office and Diabetes/Endocrinology UBTs for leading the pack!
Click here to learn more about UBTs, and to find out more about how to launch one in your department reach out to Will.Erickson@umassmemorial.org.
SHARE Updates: PCA Pathway Program, Free English Classes, and Unit Based Teams
PCA Pathway Program Now Accepting Applications

Congratulations to the first graduating cohort of the PCA Pathway Program! They’re now on-the-job as SHARE members, caring for patients at UMass Memorial.
Do you know someone who wants to begin a career at UMass Memorial working on the nursing floors? The Patient Care Associate Program is now open to friends and family of SHARE members!
A Strong Summer for Unit Based Teams
First, the bittersweet news: after helping establish the SHARE-UMass Memorial Partnership Office over the past few years, our beloved UBT Program Coordinator, Stephanie Pepi, has accepted another job at UMass Memorial. We wish you the best in Ophthamology, Steph!

There was nothing bittersweet about the recent FMCS/LERA conference in NYC, where leaders from SHARE and UMass Memorial presented to an international audience about the importance of UBTs.
U.S. Secretary of Labor Julie Su (above, middle left) even pulled the presenters into a meeting to talk about the Labor-Management projects that SHARE members are pioneering on the front lines.
SHARE members Celebrate success — and Share what they’ve Learned — at the 2024 UBT Fairs
The most exciting news for Unit Based Teams this Summer is the fantastic success of the UBT Fairs on both the Memorial and University Campuses, where SHARE members showed off their projects to over 1000 attendees. If you missed it, be sure to check out the most recent UBT Newsletter!

Click the image above for lots more photos of UBT Fair fun
Free English Classes for UMass Memorial Caregivers










Vascular Surgery Office UBT Reaches Level 4!

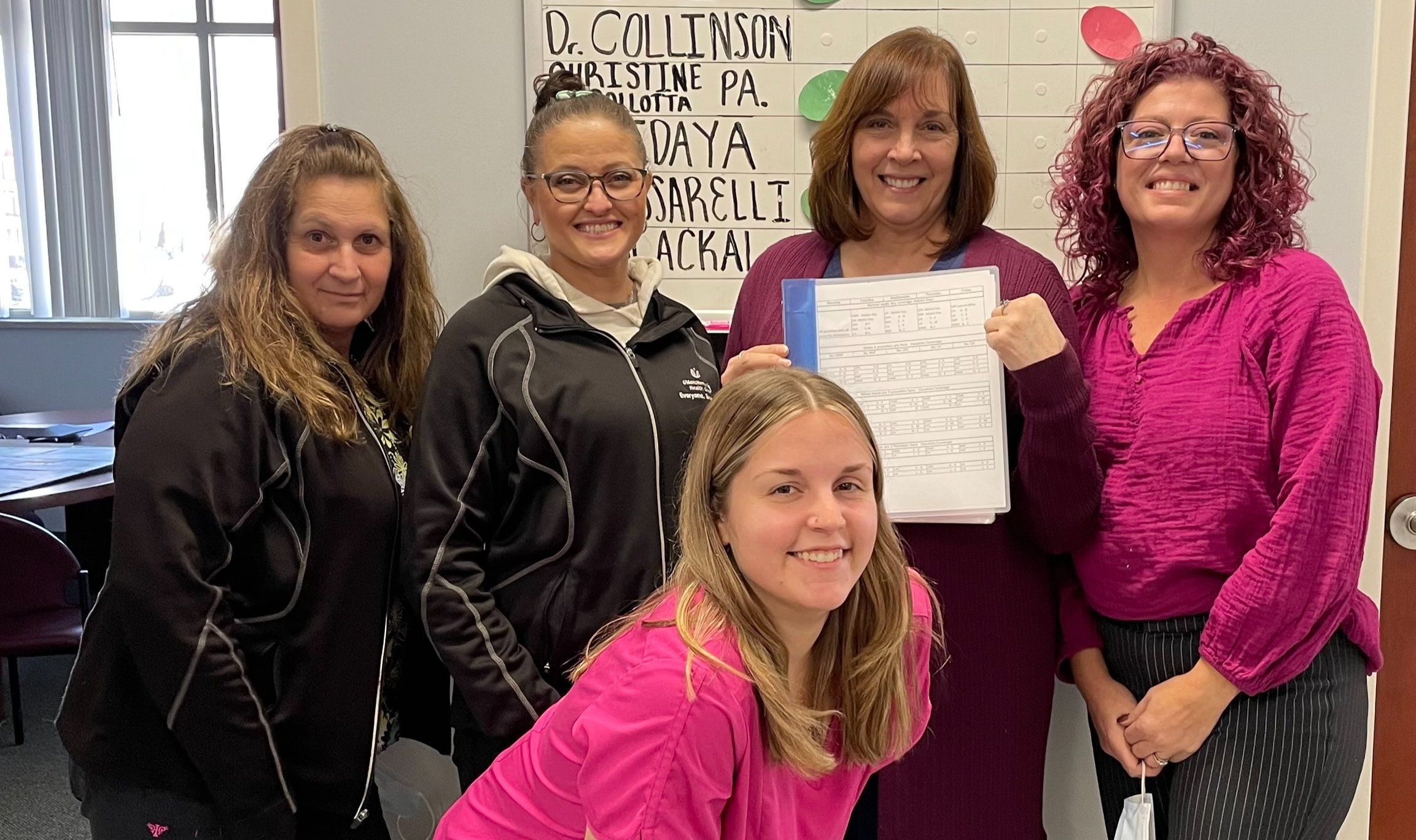
The Vascular Surgery Office UBT is among the first in the System to reach LEVEL 4 (High-Performing UBT) on their Path to Performance! That means they’ve hit some serious milestones, and established themselves as a strong team. They’ve presented their work recently to the SHARE-UMass Memorial Leadership Council (LMPC), and it’s clear that their teamwork is turning into some real fun.
Frontline SHARE members in this UBT have developed projects that have yielded measurable and sustainable improvement, and they communicate and celebrate regularly about the work and successes with the whole department.
This Unit Based Team works in the Medical School on University Campus. It is co-led by Beatrice Edmonds and Devon Germak, and is co-sponsored by Jana Hollingsworth and Stephanie Costello. The UBT Committee members include Mary Borrelli, Jeanne Magliaro, Norma Mills, Lindsey Carr and Hannah Akoto-Kesse.
Please congratulate them on their big accomplishment if you see them around!
SHARE Partnership Special: New Videos, UBTs in the National Spotlight, and More!
SHARE has designed, negotiated for, and cultivated the Unit Based Team program as a powerful way for members to be directly involved in the design of our own work. This special newsletter highlights exciting developments since the recent success of the UBT Fair.
SHARE Members on Youtube
With the help of our parent union, AFSCME, we’ve developed three short videos featuring SHARE members who describe what UBTs are, the successes they’ve had, and how the teams make a difference in their work.

All three UBT videos are now prominently featured on the SHARE homepage. Check them out! See anybody you know?
UBTs in the National Spotlight
The US Department of Labor has highlighted the Unit Based Teams in a few of their recent publications and presentations. Read more on the SHARE blog . . .
Congratulations to SHARE member Wanda Dyer, who was quoted in a recent nationwide DOL bulletin, where Wanda describes, “The Labor-Management Partnership between the hospital and the SHARE union allowed us to be involved in a Unit Based Team (UBT) where I was comfortable talking about the challenges in the workflow.
New UBT Coaches
The joint labor-management SHARE-UMass Memorial Partnership Office is growing! UBT experts Will Erickson and Stephanie Pepi have recently been joined by two new UBT Coaches: Jackie Zhou and Joan Perreault. Both have previously worked at UMass Memorial, already demonstrate exceptional skills, and we think they’re fantastic. They’re eager to help support SHARE members to make the current teams stronger and expand UBTs so that even more SHARE members can participate. Welcome Jackie and Joan! We’re excited you’re here!

Welcome to new UBT Coaches Jackie Zhou and Joan Perreault!
First Ever SHARE UBT Fair a Fantastic Success!

The first ever SHARE UBT Fair is one for the books: a brilliant event showcasing projects completed by twenty-three different teams.
Over 600 caregivers in our hospital community came to check out SHARE members’ successes and learn ways to make work better in their own departments.
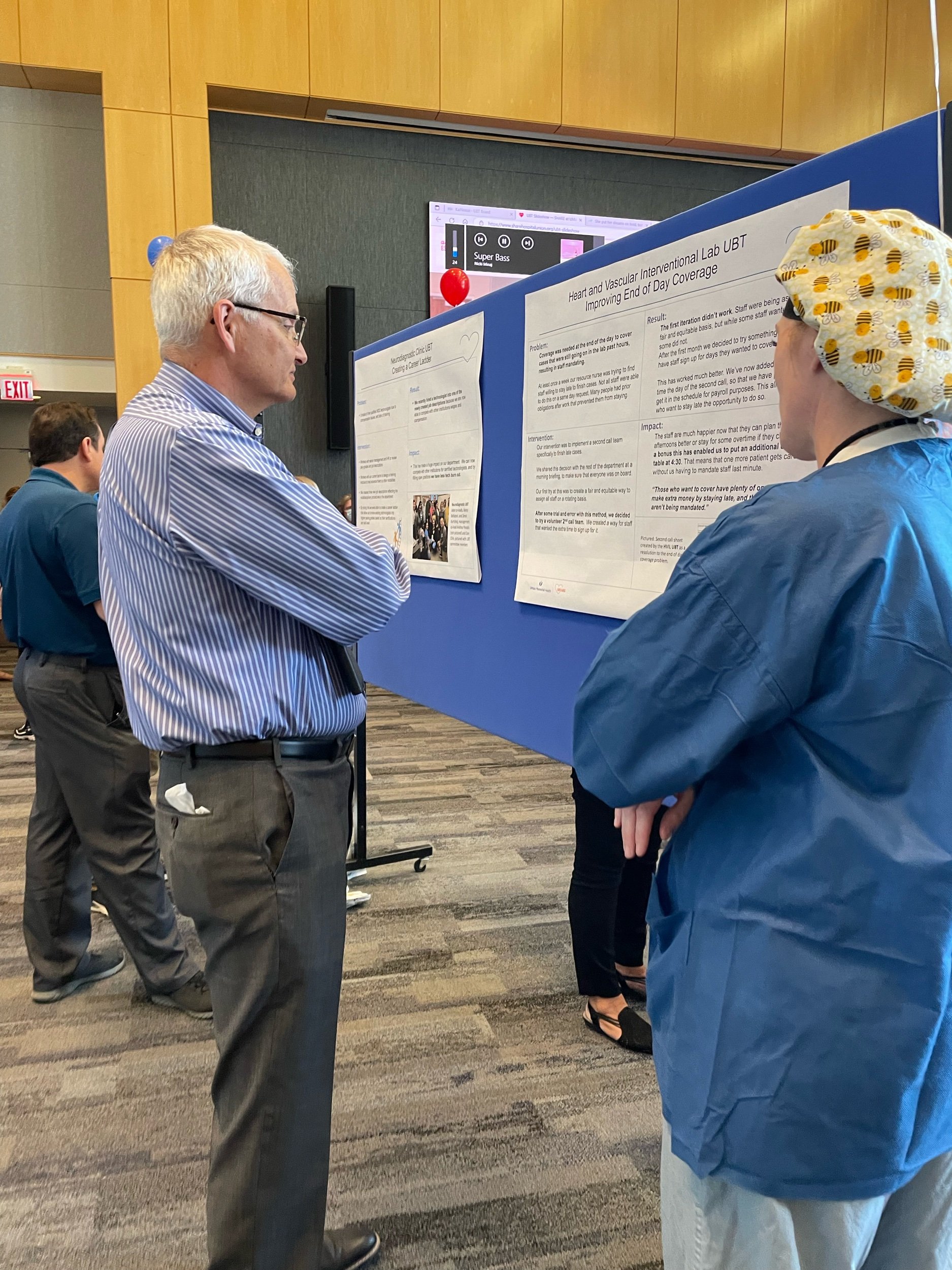
SHARE members discovered models for improving systems where they work. For example, the Neurodiagnostic Clinic developed a career ladder for staff there to grow and advance in their career, right in their own department. Seen above are NDC Co-Leads Don Chin and Zenel Kurtishaj.
Projects are designed to make the work better in a department . . . but often the results can be felt downstream, making things better for other caregivers as well.
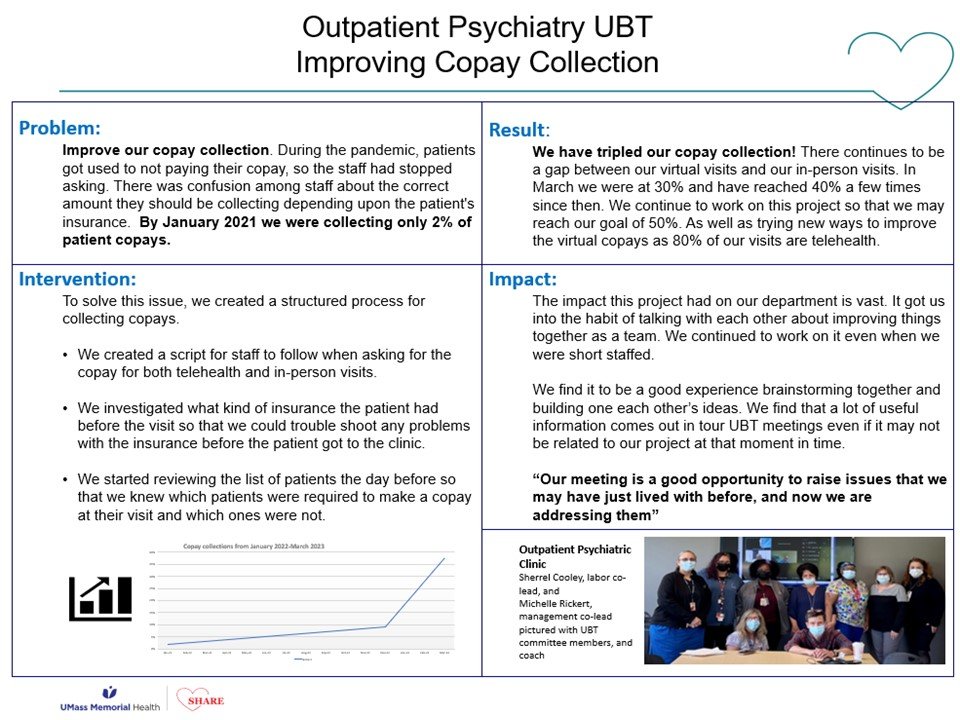
Michelle Locke (above right), management co-lead of the UBT in the Single Billing Office, appreciated the project co-lead by SHARE member Wanda Dyer of the Outpatient Psychiatry Lean Team (above left). Maximizing co-pay collections at the time of service reduces the amount of follow-up work required down the line.
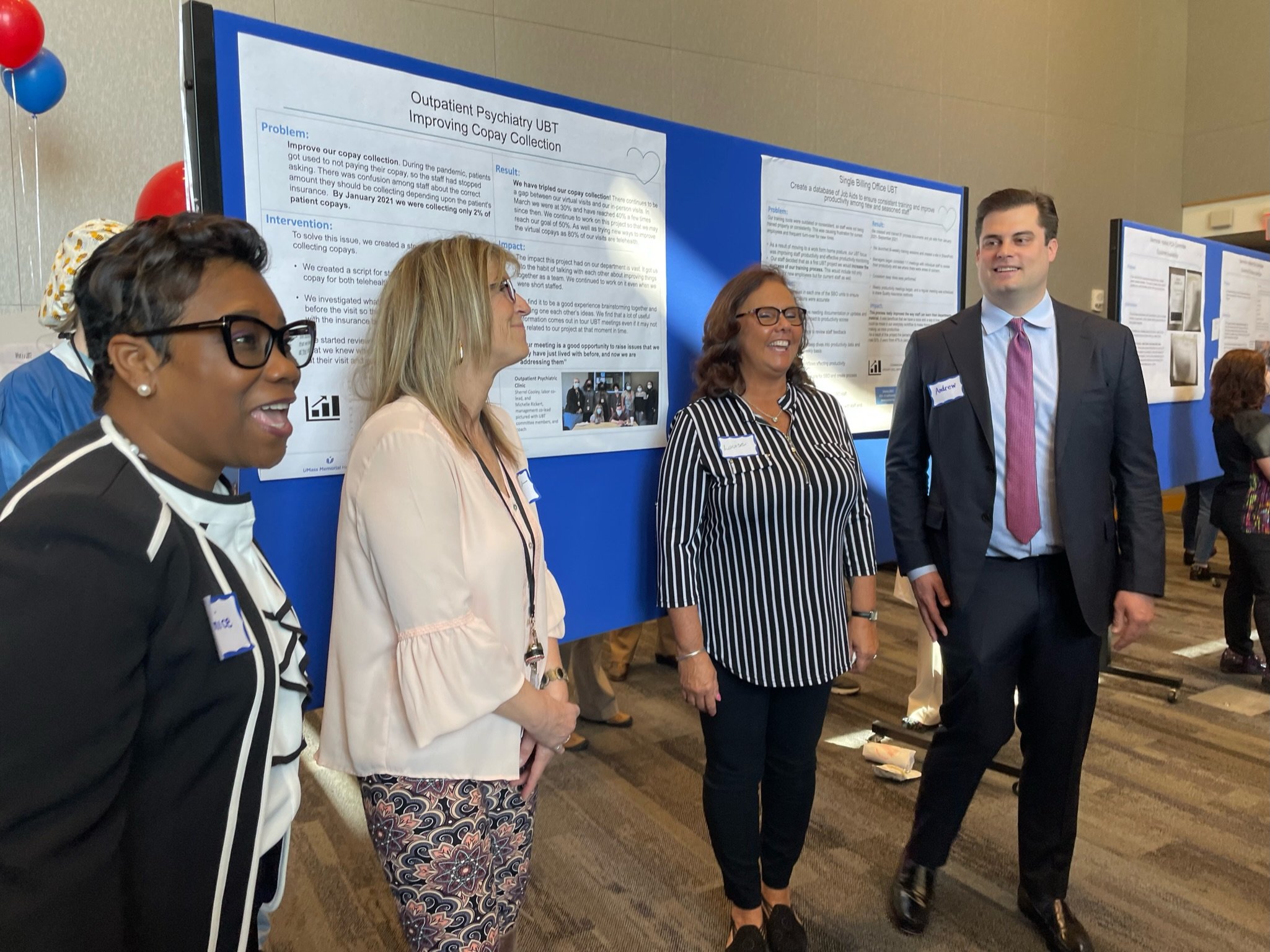
Representatives from the United States Department of Labor made the trip to see just what was going on here. Labor-Management Partnership Coordinators Darnice Marsh (above, far left) and Andrew Hasty (above, far right) are among those in federal leadership working to understand ways that Labor-Management partnerships like our own can serve as a model for broader improvements.
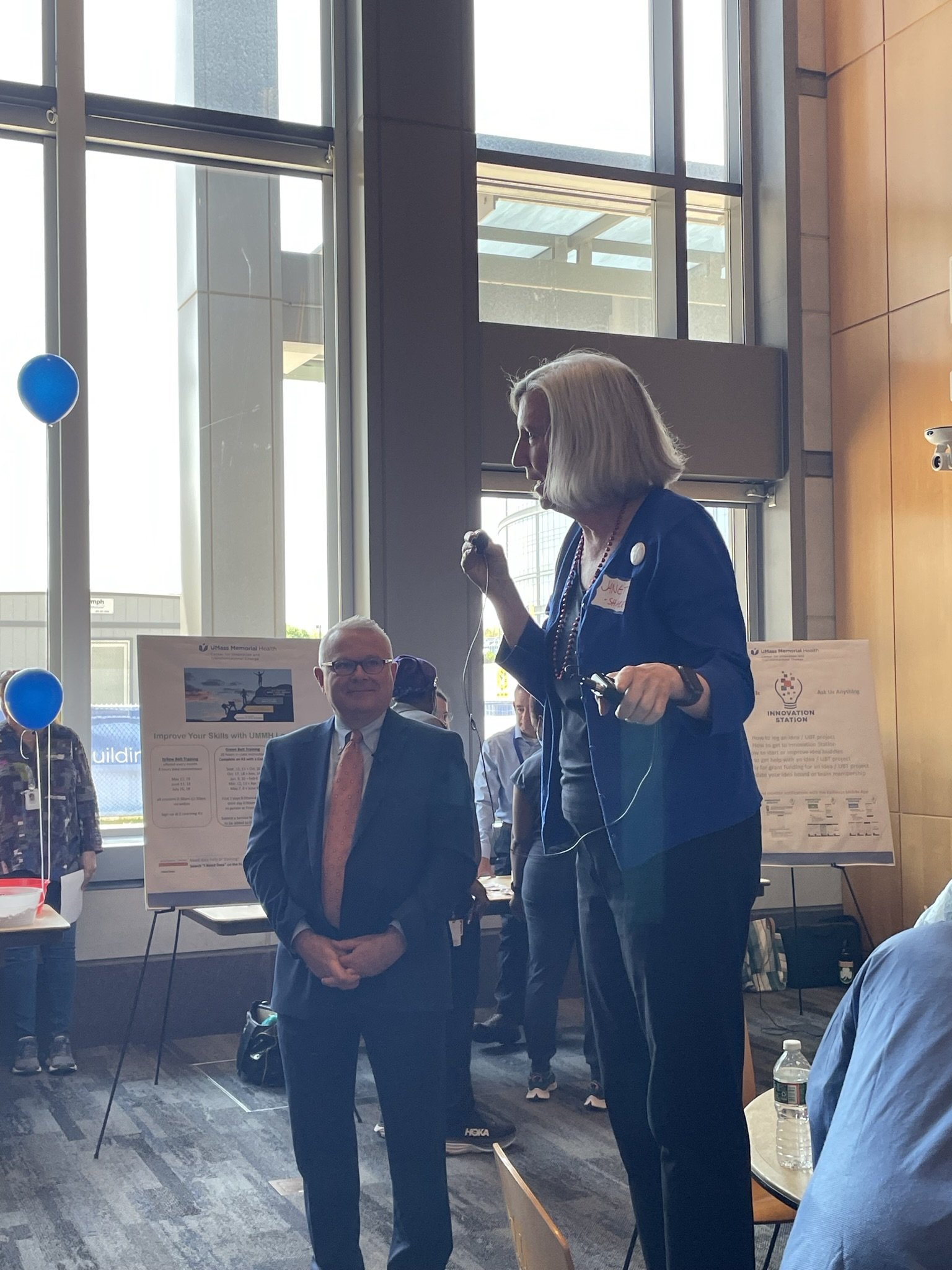
SHARE organizer Janet Wilder (standing on chair) and UMass Memorial Medical Center President Michael Gustafson (left) applauded the work of the Teams. Janet said that, during our union’s twenty-five year history, changing how it feels to come to work every day has been one of the toughest nuts for SHARE to crack . . . but UBTs have begun to do just that, and that we’re going to keep working to keep things getting better.
Incidentally, if you’ve ever been to a SHARE event before, you know that there had to be singing. This time, “The Locomotion” and “Hotel California” became victims to SHARE’s parody lyrics team.

UMass Memorial CEO Eric Dickson offered a video message of support for Unit Based Teams, citing his own belief that people closest to the work have the best ideas about how to make things better.
Dr. Dickson says that over the past ten years, the hospital system has implemented over 100 thousand frontline staff ideas, and affirms that “without reservation, the huddles that I’ve attended that are a part of the SHARE UBTs are the best in the healthcare system.”
Watch Dr. Dickson’s brief message by clicking the image above.
Everyone who came to the event was a winner, of course, but only one person could go home with the Signature SHARE Chocolate Raffle Basket. Congratulations to Nuclear Medicine Technologist (and SHARE member) Maria Nolan!
Learn more about UBTs at
www.sharehospitalunion.org/unit-based-teams
or contact
The SHARE-UMass Memorial Partnership Office
More scenes of partnership can be found online in the growing Partnership Gallery . . .





















































Barre Clinic UBT Solving the Case of the Missing Lab Orders

The Barre Clinic is at it again, having completed a second project thanks to their department’s Unit Based Team. Patients had been arriving to their lab appointments too often with no active orders to complete the labs. After brainstorming what was causing the problem and how they might best solve it, the team came up with an intervention that everyone could agree to try. Ambulatory Service Reps began checking for orders when scheduling lab appointments, and lab staff started entering orders in real-time for any outside orders that were faxed to the clinic, rather than waiting until the patient arrived.
By making these changes to their daily workflow, the staff have seen a decrease in the number of patients arriving without orders. It used to be common for patients to arrive at the lab without orders, now it is a rare occurrence.
“It cut out a lot of extra work,” says UBT Co-Lead Amy Moisan. Staff are no longer chasing down providers to get orders or ask what labs need to be drawn, and patients no longer wait in the clinic while they look for orders and enter them, saving both patients and staff precious time.
UBT Spotlight: Hahnemann Internal Medicine & The Book of Knowledge
CMG Hahnemann Internal Medicine UBT creates a Book of Knowledge for their clinic so that staff can easily access information

The Unit Based Team in Hahnemann Internal Medicine has created a way to make everyday information — as well as not so frequently asked questions — easily accessible to their staff.
The staff in the clinic found that they were wasting time looking for answers to commonly needed information. They were spending time looking through saved documents and emails to find answers to everyday questions such as accepted insurances, phone numbers, CPT codes just to name a few.
So, they gathered up the information that they had saved in various places to create a binder, or “The Book of Knowledge.” Now, each time they receive new information of value, they add it to the binder so that it is easily accessible.
It’s an uncomplicated idea with a fun, grandiose name. But coordinating this information has saved the staff a lot of time, giving them instant access to needed forms, cutting down on wait times to find information, and having everyone on the same page when giving information to their patients. “Now that we have pertinent information at our fingertips,” says management co-lead Katherine Auger, “the patients can receive correct information from all staff in a timely manner.”
